Medical Reform Committee Announces Second Implementation Plan
Establishing the Foundation for Full-scale Introduction of Regional Fees
Minimizing Criminal Liability for Medical Staff in Medical Accidents
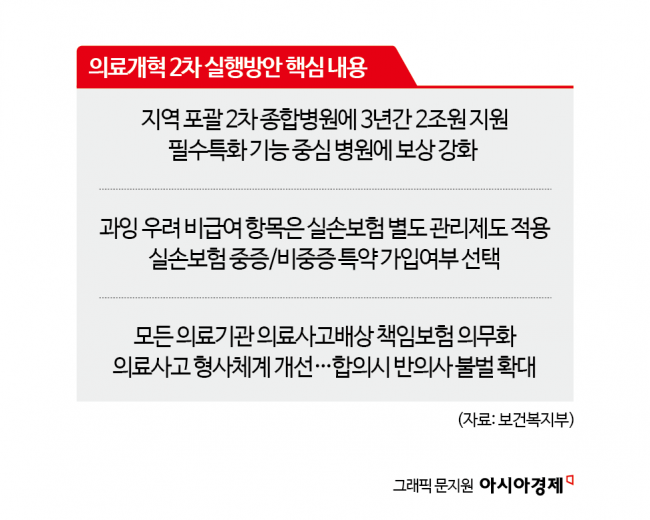
The government has decided to invest 2.3 trillion won over three years to strengthen the capabilities of regional secondary hospitals. It plans to manage excessive treatments in non-reimbursable items at an appropriate level, improve the structure and operation system of indemnity insurance products, and promote measures to reduce or exempt criminal liability of doctors for essential medical accidents without gross negligence, resulting in non-prosecution.
 Noh Yeon-hong, Chairman of the Special Committee on Medical Reform, is speaking at the 8th Special Committee on Medical Reform held on the 19th at Gwanghwamun Hall, Government Seoul Office, Jongno-gu, Seoul. Photo by Yonhap News.
Noh Yeon-hong, Chairman of the Special Committee on Medical Reform, is speaking at the 8th Special Committee on Medical Reform held on the 19th at Gwanghwamun Hall, Government Seoul Office, Jongno-gu, Seoul. Photo by Yonhap News.
The Presidential Commission on Medical Reform deliberated and approved the "Second Medical Reform Implementation Plan" containing these details on the 19th at the Government Seoul Office. While the first implementation plan announced in August last year presented urgent reform tasks focused on innovating the resident training system, supporting the structural transition of tertiary general hospitals, and improving essential medical fees, the commission explained that this second implementation plan concretizes structural reform tasks that had been delayed amid sharp conflicts of interest and various issues. The goal is to minimize avoidance of regional and essential medical care and excessive concentration of clinics, and to create an environment where all citizens can safely use medical services anytime and anywhere.
Preventing Concentration in Large Hospitals and Establishing a Regional Self-contained Medical Ecosystem
The commission first decided to strengthen the capabilities of regional essential medical care through structural transformation of regional hospital-level medical institutions. This is based on the judgment that now is the right time to enhance capabilities as tertiary general hospitals shift to focusing on severe cases and secondary hospitals’ medical services are revitalized.
To this end, the commission will actively foster "Comprehensive Secondary General Hospitals" equipped with comprehensive treatment capabilities sufficient to solve most medical problems within the region and perform essential functions such as emergency care. These hospitals will receive enhanced compensation including ▲increased fees for intensive care units ▲rewards for emergency medical procedures ▲24-hour medical support ▲performance incentives ▲introduction of regional fees. To support this, 2 trillion won will be invested over three years, with about 30% of the investment linked to performance. Additionally, a regional fee system will be actively applied and gradually expanded, which strengthens compensation where medical demand and supply are weak by utilizing regional medical maps.
Furthermore, even if a medical institution is not large in scale, if it has specialized expertise in essential treatments and properly performs essential functions such as 24-hour care, it will be restructured to provide appropriate compensation. Essential specialized functions such as ▲treatment within the golden time (heart, brain, trauma, emergency) ▲declining demand (pediatrics, childbirth) ▲cancer treatment ▲24-hour care will be designated, and a provisional "Essential Specialized Function Compensation" will be introduced with an annual budget exceeding 100 billion won.
Along with this, the commission is reviewing a reasonable adjustment of the reversal phenomenon where hospitals receive lower compensation than clinics due to the conversion factor, and a method to reflect the total increase rate of medical treatments including non-reimbursable items when contracting the conversion factor. Moreover, primary care clinics will be fostered to establish a disease prevention and integrated, continuous health management system, and patient-centered treatment capabilities suited to regional conditions will be strengthened through local medical cooperation and workforce sharing.
Premium Reduction Effect through Indemnity Insurance Non-reimbursable Riders
The commission also decided to make essential therapeutic non-reimbursable treatments reimbursable and apply a separate management system including price and treatment standards to non-reimbursable treatments with high risk of overuse, which are considered the main cause of health insurance financial deterioration.
To this end, a "managed care" category will be newly established within the selective reimbursement system, setting prices and treatment standards and applying a 95% patient co-payment rate, unlike general reimbursement. The aim is to set reasonable prices and treatment standards so that patients can use managed care items at appropriate prices while ensuring medical safety and effectiveness.
Additionally, reimbursement restrictions will be expanded in cases such as performing cosmetic or plastic surgery non-reimbursable treatments while unnecessarily combining reimbursement claims for indemnity insurance. However, medically necessary and commonly performed combined reimbursable and non-reimbursable treatments will continue to be recognized as reimbursable to prevent unreasonable patient burdens.
To ensure appropriate coverage, the indemnity insurance product structure will be reorganized, and the management and operation system of indemnity insurance products will be improved. Rationalization of the self-payment rate for health insurance reimbursable co-payments under indemnity insurance will be pursued, and coverage rationalization methods such as allowing selection of non-reimbursable severe/non-severe riders or reducing coverage limits based on the insured’s health status and medical usage tendencies will be implemented. The commission expects that if factors inducing excessive medical use among some subscribers are reduced, insurance premiums will decrease by 30-50% compared to current levels.
Recommendation for Non-prosecution in Essential Medical Accidents without Gross Negligence
The commission also proposed mandating all medical institutions to subscribe to medical accident liability insurance and developing insurance products with strengthened public functions such as special compensation for essential medical care to ensure prompt and sufficient compensation.
In particular, a reasonable premium rate system will be established for each medical institution to equalize premium rate gaps between low-risk and high-risk medical departments, and special compensation functions will be assigned to guarantee high compensation for high-risk essential treatments such as severe and emergency care. For serious incidents such as death, payment of settlement amounts through dispute mediation procedures will be mandatory.
To alleviate the insurance (mutual aid) premium burden for essential medical departments, the government will support premiums starting this year and will promote the rapid introduction of special compensation for essential medical care in the future. Expansion of coverage for force majeure accident compensation, supported by the government up to 300 million won, will also be considered.
Moreover, a provisional "Medical Accident Review Committee" involving medical professionals, consumers, and legal experts will be established to review essential medical care and gross negligence within 150 days. During the review period, summons and investigations of medical staff will be legally restrained. The committee will recommend investigation and prosecution for medical accidents caused by gross negligence but recommend refraining from prosecution for non-gross negligence, providing grounds for investigation and prosecution decisions while reducing unnecessary investigations.
Considering the high unpredictability and low avoidability of medical accidents, a "medical accident specialized judicial system" will be established where accident outcomes correspond to the degree of responsibility for the causal act. However, this will be applied on the premise of sufficient factual investigation and compensation conditions for the victim.
Accordingly, the scope of semi-conditional non-prosecution, where criminal punishment is waived if the patient and medical staff agree, will be expanded to moderate and severe injuries, and for death cases, semi-conditional non-prosecution will be applied only to essential medical acts. These measures will be decided through social consensus during the future legislative process in the National Assembly. Also, for deaths caused by simple negligence in essential medical care such as severe and emergency cases, punishment will be reduced or exempted considering the urgency at the time of the accident and rescue efforts by medical staff.
Chairman Noh Yeon-hong of the commission emphasized, "Medical reform is an urgent structural reform to solve the era’s task of strengthening regional and essential medical care. The second implementation plan, including revolutionary capability enhancement of regional hospitals, appropriate management of non-reimbursable items to prevent distortion of the medical system, improvement of indemnity insurance, and strengthening of the medical accident safety net, must be boldly and swiftly implemented to bring change to the field."
© The Asia Business Daily(www.asiae.co.kr). All rights reserved.











{kind=link}
{kind=link}