Introduction of Public Policy Fee in Emergency and Essential Medical Care
Institutions Reorganized Based on 'Final Treatment Capability' Assessment
Simultaneous Promotion of Medical Workforce Attraction and Supply Expansion
 President Yoon Suk-yeol is receiving a briefing on the Ministry of Health and Welfare's work at the presidential office in the Yongsan Presidential Office building in Seoul on August 19.
President Yoon Suk-yeol is receiving a briefing on the Ministry of Health and Welfare's work at the presidential office in the Yongsan Presidential Office building in Seoul on August 19. [Image source=Yonhap News]
[Asia Economy Reporter Kim Young-won] The government has decided to enhance fiscal soundness by limiting the previously uniformly expanded coverage for procedures such as Magnetic Resonance Imaging (MRI), and to invest the saved resources into essential medical services. On the 8th, the Ministry of Health and Welfare held a public hearing at the President Hotel in Jung-gu, Seoul, to announce the 'Measures to Enhance the Sustainability of Health Insurance and Support Essential Medical Services.'
The Ministry judged that despite large-scale financial input for strengthening health insurance coverage, the imbalance in the medical system, such as concentration in large hospitals in the metropolitan area, has worsened, and efforts to support essential medical services have been insufficient. This year, more than 50% of the 67 pediatric cancer specialists nationwide, totaling 41, are concentrated in the Seoul and Gyeonggi regions. Following the recent incident where a nurse at Seoul Asan Medical Center collapsed and died from a cerebral hemorrhage while on duty, the Ministry announced plans to expand essential medical services.
Accordingly, the government plans to reduce health insurance finances through re-examination of coverage application and invest these funds into essential medical services and catastrophic medical expense support. Strengthening essential medical services and catastrophic medical expenses are also included in the Yoon Suk-yeol administration's national agenda.
Introduction of 'Public Policy Fee'... Appropriate Compensation for Essential and Emergency Medical Services
The government will introduce a public policy fee system to provide appropriate compensation for essential medical services. The public policy fee system is a scheme that assigns separate fees to institutions responsible for public medical functions to strengthen the compensation system. The aim is to strengthen the foundation of essential medical services by introducing public policy fees in areas that are avoided, such as craniotomy for cerebral aneurysm, and in areas with decreasing demand, such as childbirth. This complements the difficulty of providing appropriate compensation in low-frequency, high-risk essential medical fields under the fee-for-service system, where revenue increases only by increasing the volume of services.
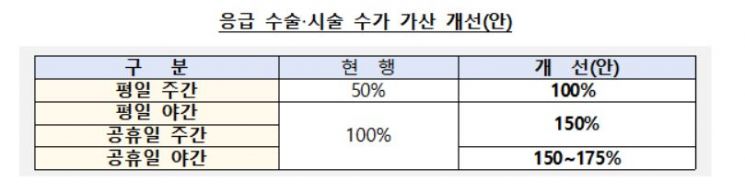
First, the fee add-on rates for emergency surgeries and procedures performed at night and on holidays, such as cerebral aneurysm and severe trauma, will be increased. Currently, the weekday daytime fee add-on is 50%, which will be raised to 100%, and the weekday nighttime and holiday fee add-ons will be expanded from 100% to 150-175%. This will be applied first to 40 regional emergency medical centers and 18 tertiary general hospitals, with plans to expand to more institutions as the emergency medical system is reorganized.
To ensure follow-up care for severe patients visiting emergency rooms, a new 'Emergency Room Dedicated Admission Management Fee' will be established. Until now, management fees were calculated only when admitted to emergency-dedicated intensive care units, but management fees will also be calculated for admissions to emergency-dedicated wards.
Additionally, the fee criteria will be subdivided to reflect the difficulty and resource input level, and additional compensation will be provided for high-difficulty and high-risk medical procedures. For example, when performing surgery for congenital anomalies of the pediatric ventricle and great vessels, the same fee was applied regardless of difficulty, but additional compensation will be given when applying high-difficulty surgical methods. The government plans to first apply additional compensation in the cardiovascular and cerebrovascular disease fields and then expand it.
To maintain the foundation of essential medical care such as childbirth and pediatrics in medically vulnerable areas, additional fees for vulnerable areas and personnel and safety policy fees will be provided. In cities, counties, and districts excluding metropolitan cities, an additional 'vulnerable area fee' equivalent to 100% of the current childbirth fee is paid. Furthermore, reflecting disputes related to unavoidable medical accidents, an additional personnel and safety fee equal to 100% of the childbirth fee is added, which is three times the current childbirth fee. In addition, during infectious disease crises, an 'infectious disease policy fee' will add another 100% of the childbirth fee.
To maintain the treatment base for severe pediatric patients, a pilot project will be conducted to compensate deficits of children's public specialized medical centers retrospectively, and compensation for home treatment and short-term hospitalization of pediatric patients will also be strengthened.
Promotion of Regionally Conclusive Essential Medical Services Without Unnecessary Emergency Room Transfers
To provide 'regionally conclusive essential medical services,' the government plans to reorganize 40 regional emergency medical centers into severe emergency medical centers equipped with final treatment capabilities such as surgeries and procedures. This aims to strengthen timely treatment functions so that severe and emergency patients can receive final treatment without being transferred to other hospitals. Additionally, the number of severe emergency medical centers will be expanded to around 50 by 2025 to respond to the golden time within living quarters when severe emergency patients occur.
As a way to effectively utilize limited medical personnel and institutions, a cooperative system among medical institutions within the region was proposed. The government plans to strengthen the 'Emergency Transfer Cooperative Network' system, which surveys emergency medical resources by region centered on local governments and updates institutions and personnel capable of final treatment for each emergency disease.
Im In-taek, Director of Health and Medical Policy at the Ministry of Health and Welfare, said, "Until now, emergency rooms were designated based only on emergency capabilities, but from now on, emergency rooms will be designated based on the hospital's final treatment capabilities for cardiovascular diseases, severe trauma, etc. We will prevent cases where patients are transferred to other hospitals due to insufficient treatment capabilities in emergency rooms." He added, "Regional cardiovascular and cerebrovascular centers will also be reorganized to focus on specialized treatments such as high-difficulty surgeries, and those that do not meet these capabilities will be decisively excluded."
The government also emphasized its stance to secure sufficient medical personnel. Considering that it takes more than 10 years to train new specialists, it plans to induce personnel inflow through improved working conditions and balanced placement while expanding the total amount of specialized personnel to increase supply.
To induce personnel inflow, the government plans to improve the workload and treatment of personnel in essential medical fields. By analyzing working conditions by field and region, it will improve systems related to doctors' on-call duties and working hours, and promote the introduction of the '(tentative name) Korean Doctor Award' for medical personnel dedicated to essential medical fields. To reduce regional personnel disparities, the assignment of residents outside the metropolitan area will be expanded, and resident dispatch training between national university hospitals and local medical centers will be activated.
Regarding the expansion of doctor supply, the government intends to continue discussions with the medical community. In September 2020, the government and medical organizations agreed to discuss the expansion of doctor quotas after the stabilization of COVID-19. Cha Jeon-gyeong, Director of Health and Medical Policy Division at the Ministry of Health and Welfare, said, "We will proceed with the principle of consultation and aim to resume discussions through the medical-government consultative body."
Going forward, the government plans to continuously identify essential medical fields requiring support, prepare additional measures, and establish the 'Health and Medical Development Plan (2024-2028)' to present mid- to long-term health and medical policy directions, including the reorganization of the medical delivery system.
© The Asia Business Daily(www.asiae.co.kr). All rights reserved.
![Clutching a Stolen Dior Bag, Saying "I Hate Being Poor but Real"... The Grotesque Con of a "Human Knockoff" [Slate]](https://cwcontent.asiae.co.kr/asiaresize/183/2026021902243444107_1771435474.jpg)











{kind=link}
{kind=link}