Announced Major Shift Immediately After Seol Holiday
Separating Movement Paths, Partitions, and Specimen Collection Spaces
Will Take Time to Fully Secure
"Medical Fees Must Be Realistic to Encourage Participation"
 On the morning of the 27th, Lee Jeong-geun, the full-time vice president of the Korean Medical Association, is speaking at the 'Press Conference on Operation Plans for COVID-19 Clinics' held at the Korean Medical Association's temporary Yongsan office in Yongsan-gu, Seoul. [Image source=Yonhap News]
On the morning of the 27th, Lee Jeong-geun, the full-time vice president of the Korean Medical Association, is speaking at the 'Press Conference on Operation Plans for COVID-19 Clinics' held at the Korean Medical Association's temporary Yongsan office in Yongsan-gu, Seoul. [Image source=Yonhap News]
[Asia Economy reporters Lee Gwan-ju and Lee Chun-hee] After the Lunar New Year holiday, the COVID-19 response system will change significantly, focusing on local clinics. Due to the surge in new confirmed cases caused by the spread of the Omicron variant, diagnosis, treatment, and prescriptions will be entrusted to primary clinics and hospitals with good accessibility. On the 28th, Prime Minister Kim Boo-kyum said at the Central Disaster and Safety Countermeasures Headquarters meeting, "From right after the Lunar New Year holiday, people will be able to get COVID tests and treatment at nearby local clinics and hospitals," adding, "This completes the last piece of our quarantine and medical response strategy against Omicron." The key is participation rate. Many local clinics must participate in COVID-19 treatment to improve patient accessibility and prevent the spread of infection.
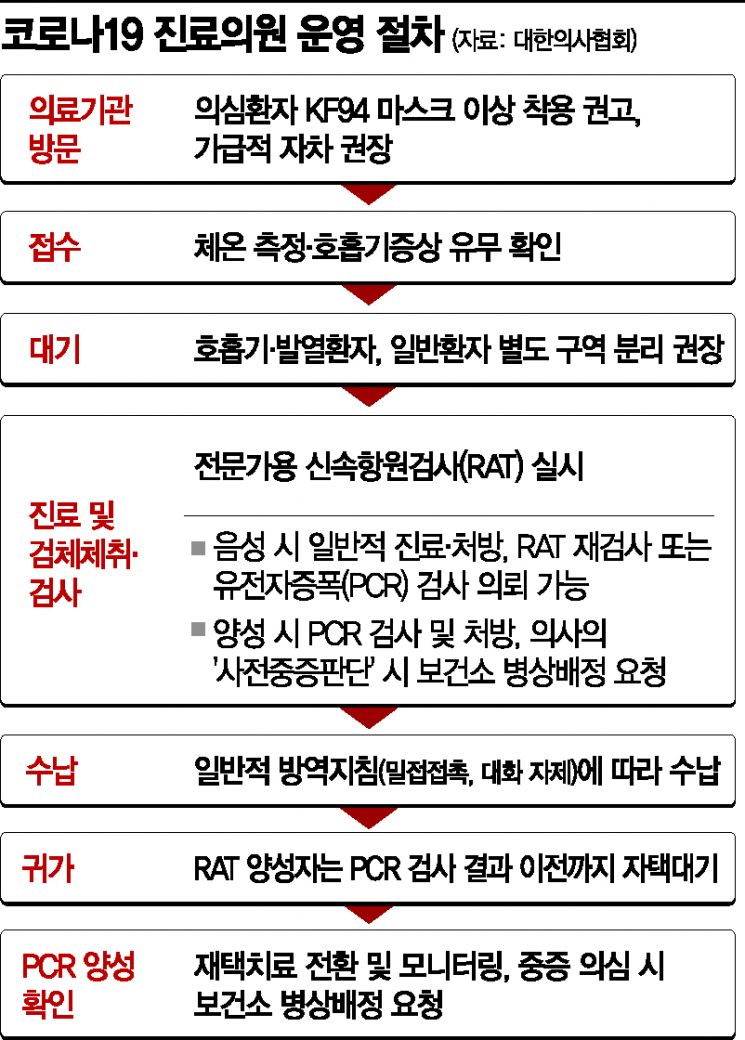
◆Many local clinics are unprepared= Starting from the 3rd of next month, right after the Lunar New Year holiday, the COVID-19 diagnosis and treatment response system will shift to focus on local clinics and hospitals. Until now, if COVID-19 was suspected, people visited screening clinics set up at local public health centers to receive polymerase chain reaction (PCR) tests, and if tested positive, they were treated at home, in residential treatment centers, or transferred to dedicated hospitals based on health authorities' decisions. This will change to a system where local clinics take the lead in diagnosis, treatment, and prescriptions based on professional rapid antigen tests (RAT).
The problem is the participation rate. The medical community expects that not many clinics will be ready to immediately engage in diagnosis and treatment right after the holiday. Previously, health authorities announced that about 360 clinics are participating in home treatment management. There are only 431 respiratory specialist clinics nationwide with COVID-19 treatment experience. Initial confusion is virtually unavoidable. The core of the Korean Medical Association's 'COVID-19 Clinic Operation Plan' announced the day before is infection prevention within medical institutions, such as separating patient flow and installing partitions. However, due to the nature of local clinics, waiting rooms are often small, and many lack separate spaces for specimen collection, so preparing these will inevitably take time.
The Medical Association plans to encourage at least 1,000 medical institutions to participate in COVID-19 diagnosis and treatment. Lee Sang-woon, vice president of the Medical Association, said, "Currently, applications are being received mainly through the medical associations of 16 cities and provinces, collected by the Medical Association, and registered all at once with the Health Insurance Review and Assessment Service," adding, "Although it is difficult to say exactly how many medical institutions are expected to participate, the goal is for up to several thousand institutions to participate so that people nationwide can visit clinics and hospitals without geographical difficulty."
There are also calls for medical fees to be adjusted realistically to increase participation rates. Currently, the RAT fee is being discussed around 55,000 won, citing vulnerability in infection control. A Medical Association official said, "Various unexpected situations can arise in infection control," adding, "Since it is not simple to manage patient prognosis and underlying diseases, we are suggesting the need for a fee increase."
◆Concerns about ‘reinfection’ amid Omicron pandemic= As the Omicron variant spreads, concerns about reinfection have increased even for those who have already been infected with COVID-19. According to the 'Domestic COVID-19 Reinfection Case Status' announced by the Korea Disease Control and Prevention Agency (KDCA) the day before, there have been a total of 142 reinfection cases in Korea since the outbreak. Of these, a staggering 85.9% (122 cases) occurred after July last year, when the Delta variant became dominant. There were three severe cases due to reinfection, two of whom died. All of them were unvaccinated. The risk of reinfection was 0.34 times lower for those who had received the first and second doses of the vaccine compared to the unvaccinated.
The KDCA attributes these reinfections to the high transmissibility of the Delta variant. The Omicron variant is understood to be more than twice as transmissible as Delta. Recent analysis from the UK showed that the reinfection rate during the Omicron wave was 16 times higher than during the Delta wave. The KDCA emphasized, "Omicron is also reported to have a high possibility of reinfection," and stressed, "Vaccination completion should be actively encouraged to suppress and prevent reinfection."
© The Asia Business Daily(www.asiae.co.kr). All rights reserved.
![User Who Sold Erroneously Deposited Bitcoins to Repay Debt and Fund Entertainment... What Did the Supreme Court Decide in 2021? [Legal Issue Check]](https://cwcontent.asiae.co.kr/asiaresize/183/2026020910431234020_1770601391.png)











{kind=link}
{kind=link}