Lee Guk-jong - Ajou University Hospital, Said to Be Years of Accumulated Conflict
Fact-Checking the Background of the Conflict Surrounding Trauma Center Operations

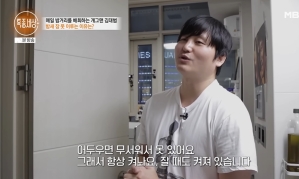
[Asia Economy Reporter Choi Dae-yeol] "The severe trauma center project in Korea is sinking. It just hasn't been visible on the surface. (Omitted) Many people say that building a severe trauma medical system is necessary, but everyone only tries to enforce their own interests, and no one genuinely studies what a severe trauma center really is overseas."
"'If you think there are so many problems, then just close the trauma center and return the project.' I was horrified by the organization's management style that, without official resolution, used various coercive remarks to induce me to resign voluntarily." (Excerpt from Lee Guk-jong's 'Golden Hour 2')
Professor Lee Guk-jong of Ajou University Hospital, who leads the Southern Gyeonggi Regional Trauma Center, wrote this book in 2018 as an autobiographical account about himself and those around him, as well as a record showing how the domestic trauma center system has evolved. Professor Lee, who started his career in trauma surgery in 2002, returned after overseas training in the U.S. and the U.K., and for over a decade, he devoted himself to explaining why trauma centers?which were then a novel concept?were necessary, how they should be operated, and how important such work was.
He conveyed that conflicts had existed for years, both within the hospital and in the external perception of trauma centers. He believed that operating trauma centers solely through the blood, sweat, and dedication of staff was unsustainable and likely to result in unhappiness for everyone involved.
Fact Check ① Are Trauma Centers the Main Cause of Hospital Deficits?
It varies by hospital with regional trauma centers, so it is difficult to generalize. According to an analysis by the Korea Health Industry Development Institute under the Ministry of Health and Welfare in 2017, the profit and loss of trauma centers at Ajou University, Pusan National University, and Ulsan University Hospitals showed a loss rate of 40-50% when subsidies were not considered. At Ajou University Hospital, the cost was about 31 billion KRW, with revenue of 21 billion KRW, resulting in an estimated loss of around 10 billion KRW.
However, since then, institutional support has improved with increased funding for medical staff and additional fees for trauma patients, leading to a general consensus that conditions have improved compared to the past. Professor Lee also stated in a media interview, "(The trauma center) is not the main cause of deficits, nor is it actually running at a loss, but it is being treated as an unnecessary organization, which makes the hospital think it should no longer operate the center."
 Professor Lee Guk-jong of Ajou University Hospital and Deputy Minister Lim Seo-jeong of the Ministry of Employment and Labor are seen talking at the '2019 Asia Women Leaders Forum' hosted by Asia Economy in October last year. Professor Lee discussed the poor treatment of nurses caring for critically ill patients at that time.
Professor Lee Guk-jong of Ajou University Hospital and Deputy Minister Lim Seo-jeong of the Ministry of Employment and Labor are seen talking at the '2019 Asia Women Leaders Forum' hosted by Asia Economy in October last year. Professor Lee discussed the poor treatment of nurses caring for critically ill patients at that time. Photo by Moon Ho-nam munonam@
Fact Check ② Will Increasing Budget Support Improve the Situation?
Regional trauma centers are established when hospitals apply and meet certain criteria, with the government approving and providing installation and operational funding. The budget used by the government to build a severe trauma specialized treatment system was about 52.1 billion KRW in 2018 and approximately 64.6 billion KRW last year. This year, it is about 61.5 billion KRW. The decrease is mainly due to reduced operational support budgets for regional trauma centers, which make up most of the support budget. In recent 3 to 4 years, budget execution rates have been only 60-70%, causing budget shrinkage. The trauma centers still face avoidance issues on the front lines due to the high intensity of work.
Simply put, there is money to give, but no personnel to spend it. Stories from Professor Lee and center members include staying at the hospital for meals and lodging, going home only about four days a year, nurses who had to ride helicopters or care for patients despite pregnancy, illness, or injury due to lack of substitutes. In Professor Lee's words, the trauma center barely managed to operate because individuals were "squeezed and worked to the bone." Considering that government or local government budget support increases administrative tasks for the department, expanding budget support may be welcomed by hospital management but is unlikely to be what frontline workers want.
Fact Check ③ The Number of Regional Centers Was Not Originally 17
The Ministry of Health and Welfare initially planned to divide the country into 5 or 6 regions and build large-scale centers at the level of Level 1 trauma centers in the U.S. Level 1 refers to facilities and personnel equipped to treat severely injured trauma patients. However, due to opposition from budget authorities citing low economic feasibility and other factors, the plan was adjusted to split into 17 smaller centers operating at a somewhat lower level than Level 1. Professor Kim Yoon of Seoul National University College of Medicine, who was involved in the early research, said, "The Ministry of Health and Welfare has never officially explained this."
Compared to the original plan, the total number of centers increased, but the size of each center decreased. Inevitably, this structure increased dependence on the main hospitals applying for the regional trauma center project. Professor Lee also experienced years of conflict with hospital management over issues such as emergency helicopter operations and medical staff management while operating the center under this dependence. Even when Professor Lee emphasized the common-sense principle of "treating the sick," hospital management often refused, citing "resource allocation efficiency."
© The Asia Business Daily(www.asiae.co.kr). All rights reserved.












{kind=link}
{kind=link}